I decided to peruse some of the older posts, perhaps in reflection of the road we’ve traveled so far. So, I found this, and I wanted to repost it….Comparing some of the activities and insights from then (Friday, March 28, 2014) until now it’s interesting, and a little sad. However, the girl is still hanging in there despite her lack of eating, or want of more calories (I checked - her shakes are about 200 calories, so with everything else, she’s probably taking on less than 400 a day), which demonstrates great will and fortitude! I hope it doesn’t end with her generation...But, if you’d care to, please read on:
When Mom's buddy, Nadya, sent me the literature on LBD, I read it, but it didn't make sense. It was too vague. I can't say it isn't still a little vague, but it's becoming clearer as to what it is, how it manifests (at least in Mom), and what more to expect.
Lewy Body Dementia (LBD)
Lewy body dementia (LBD) is one of the most common types of progressive dementia. Lewy body dementia usually occurs sporadically, in people with no known family history of the disease. However, rare familial cases have occasionally been reported. In Lewy body dementia, cells die in the brain's cortex (outer layer), and in a part of the mid-brain called the substantia nigra. Many of the remaining nerve cells in the substantia nigra contain abnormal structures called Lewy bodies that are the hallmark of the disease.
The symptoms of Lewy body dementia overlap with Alzheimer's disease in many ways, and may include memory impairment, poor judgment, and confusion. However, Lewy body dementia typically also includes visual hallucinations, parkinsonian symptoms such as a shuffling gait (walk) and flexed posture, and day-to-day fluctuations in the severity of symptoms. Patients with Lewy body dementia live an average of 7 years after symptoms begin. There is no cure for Lewy body dementia, and treatments are aimed at controlling the parkinsonian and psychiatric symptoms of the disorder.
Thanks to sites such as:
Among others, I have been able to process and determine more of what to expect.
Here is a portion of an article on using MRI scanning to determine something about dementia -
CT scans and MRIs are helpful tools physicians use to examine structural brain changes. These scans are useful in detecting strokes, tumors, head injury and other structural changes including hydrocephalus, which can cause of dementia. MRIs provide superior images compared with CT scans in detecting structural problems in the brain.
Some of the causes of dementia that can be detected well by an MRI include brain tumors, vascular dementia/multi-infarct dementia (dementia caused by multiple strokes), normal pressure hydrocephalus, or Creutzfeldt-Jakob disease — a type of infectious disease in humans related to bovine spongiform encephalitis or “mad cow disease”).
It can be very difficult to differentiate between types of dementia in the doctor’s office since many disorders can initially present with similar symptoms. Most degenerative causes of dementia such as Alzheimer’s disease and LBD are characterized by atrophy or shrinkage of the brain due to cell death. However, the patterns are similar so that the MRI cannot distinguish between Alzheimer’s and LBD but can provide supporting evidence that the patient’s symptoms are not due to another structural lesion. This is important because some causes of dementia such as hydrocephalus and brain tumors are potentially reversible if caught and treated early.
In the early stages of LBD the atrophy can be very subtle. In the more advanced stages of dementia, the atrophy can be quite severe. Researchers are actively studying whether the pattern and progression of brain atrophy in LBD can lead to better understanding of disease mechanisms and improved diagnosis.
- See more at: http://www.lbda.org/feature/5203/brain-imaging-for-lewy-body-dementia.htm#sthash.bzO9BB3m.dpuf (lbda.org, 2014).
What isn't said here is that there cannot be any true determination, really, until an autopsy is performed after death, to inspect the brain and verify the diagnosis.

Here is an illustration of the brain.

These are forms of dementia, to help better illustrate what types there are for all of us who are not quite sure.
Thanks to http://www.medicinenet.com/dementia_pictures_slideshow/article.htm for all this help!
What Causes Dementia?
All forms of dementia result from the death of nerve cells and/or the loss of communication among these cells. The human brain is a very complex and intricate machine and many factors can interfere with its functioning. Researchers have uncovered many of these factors, but they have not yet been able to fit these puzzle pieces together in order to form a complete picture of how dementias develop.
Many types of dementia, including Alzheimer's disease, Lewy body dementia, Parkinson's dementia, and Pick's disease, are characterized by abnormal structures called inclusions in the brain. Because these inclusions, which contain abnormal proteins, are so common in people with dementia, researchers suspect that they play a role in the development of symptoms. However, that role is unknown, and in some cases the inclusions may simply be a side effect of the disease process that leads to the dementia.
Genes clearly play a role in the development of some kinds of dementia. However, in Alzheimer's disease and many other disorders, the dementia usually cannot be tied to a single abnormal gene. Instead, these forms of dementia appear to result from a complex interaction of genes, lifestyle factors, and other environmental influences.
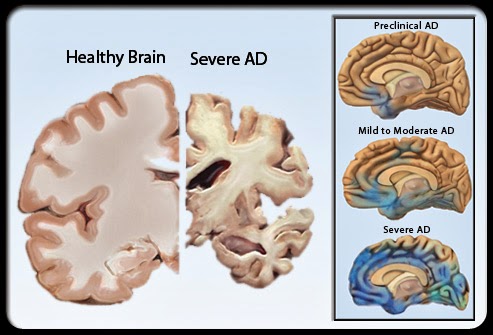
Here is a comparison between a healthy brain and one with Alzheimer's, or dementia.

This gets a little more inside - showing what happens to the brain when afflicted.

Here's what the little bastards look like, that afflict the brain and the neurons in Mom's head.
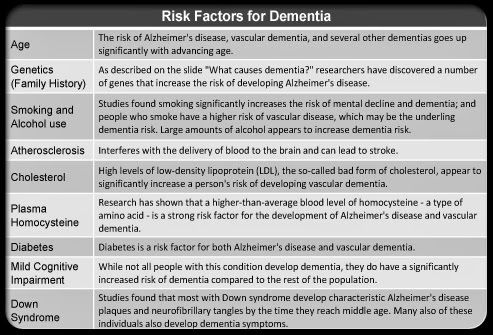
AT this time, here's an example of who might be at risk....If this is of help, to you, then I'm glad.
The ironic component to Mom having this is her Mother had Alzheimer's. Our grandmother was diagnosed in September 1983 and died in April 1984. I know this through Mom's journals, and her introspection on the diagnosis. Mom was upset that this could have been possible.
One of Mom's cronies told me that for their generation this was quite embarrassing, and indeed, for Mom, it is. She will not admit there is anything wrong, although she knows it is. My brother, Tom, and I both gently remind her from time to time (as he lives and works in Seattle, and isn't able to visit too often, but does try to make it once a month; they provide her with movies, a television - which she refuses to allow to be set up, clothes, and outings). She understands, but then retreats back into denial within a short time.
Mom is able to do her crosswords, pretty well. And her good friends, Connie and Jean, come to play Scrabble with her almost weekly - of course, Mom creates rules that they try to abide by, but there are times...Thank God they have a sense of humor and quite a lot of patience. Mom is quite competitive, and loves winning. I do believe, though, that she has won the vast majority of games.
This keeps Mom's brain active and alert. However, she has troubles distinguishing between dreams and reality. In a letter to my father, which she wrote recently (yes, she writes letters to him, her parents, and she wrote one to her grandparents, as well - luckily I take all her mail and post it so I can catch all this) she told him I had related a family gathering in which he was there but she wasn't invited. She was not happy and was quite depressed by this. Well, such a thing never occurred.
Connie and Jean tell me Mom seems fine and functional about 92% of the time. But for me, she operates about 50% of the time in reality, and the rest is in somewhere else. She tells stories about the family, while engaging, which are not based on fact or even remotely true. These stories continue to grow, little by little, into miniature sagas.
Just the other day, she began tremoring in her left arm. It wasn't about angst or worry - it just happened. This is significant. I'm hoping syncope and falling are not coming soon, along with rigidity (although she has stated she has fallen for no reason, but doesn't want anyone to know).
Well, that's all for now. I hope this was helpful and a little enlightening.
I placed my sources at the head, in case you were wondering where to go for more information.













